
Pulmonary sequestration (Sequestration)
General information:
- Mass of nonfunctioning lung tissue that lacks an obvious communication with the tracheobronchial tree and that receives it arterial blood from the systemic circulation. The venous drainage is either into the pulmonary vein (large shunts may develop; > 30% of cardiac output: cyanosis, clubbing of the fingers, dyspnea; risk of hemotothorax and hemopthisis) or the vena azygos.
- Sequestrations are classified basically as:
- Interlobar: The sequestration is located within the normal lung. According to the blood supply interlobar sequestrations are divided according to the Pryce classification (arterial blood supply and the ventilation pattern) into:
.) Type I: Regularly ventilated lung tissue perfused by two arterial blood supplies (pulmonary artery, systemic artery).
.) Type II: Sequestrated, irregularly ventilated (atelectatic) lung tissue perfused by two arterial blood supplies on the margins (pulmonary artery, systemic artery).
.) Type III: Sequestrated, not ventilated lung tissue perfused only by the systemic artery blood supply.
- Extralobar: The sequestration is completely separated as an accessory lobe from the normal lung (Rokitansky lobe). Associated with other abnormalities (diaphragmatic hernia). Arterial blood supply usually from the abdominal aorta, the venous blood usually returns into the azygos vein.
- More than two thirds are located in the lower lobes.
- Two thirds of the sequestrations are on the left side.
- More than two thirds get their arterial blood supply from the abdominal aorta (large vessel passing the diaphragm in the hiatus aortae. The most specific diagnostic criterium for sequestration. The atypic artery is detectable by angio – CT or by Doppler – ultrasound).
- More than two thirds have only one arterial supporting vessel.
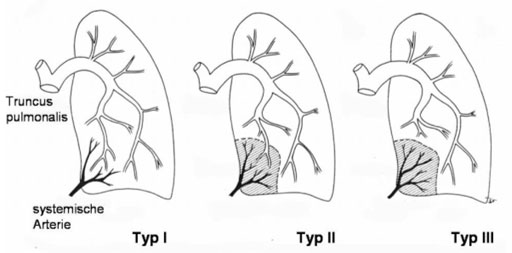
Intralobar sequestrations; Pryce classification (Bettex M. et. al. : Kinderchirurgie, Thieme 1982)
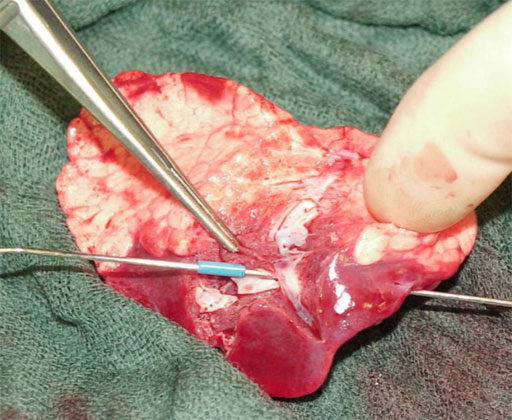
Type II of intralobar sequestration (surgically opened large arterial vessels)
Symptoms:
- Small extralobar sequestrations may be completely asymptomatic.
- Interlobar sequestrations tend to provoke infections (non-functioning lung tissue and the compressed surrounding lung tissue). Children with unexplained recurrent pneumonias must be suspected of having sequestration.
- Hemothorax, hemopthisis.
Diagnostic workout:
- Prenatal ultrasound.
- High resolution CT and angiographic CT (abnormal arterial blood supply detectable at the level of the diaphragm).
- Angiography or MRI (needs general anesthesia).
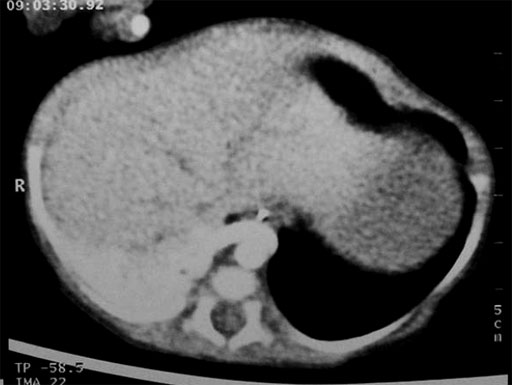
Abnormal arterial blood supply of the sequestration
Indication for operation:
- Clear indication for resection.
Treatment/Operation:
- Interlobar sequestration: lobe resection.
- Extralobar sequestration: simple resection.
- In all types of resections the feeding transdiaphragmatic artery has to be handled very carefully (the vessel can retract itself below the diaphragm causing a massive and extremely dangerous bleeding; splitting incision of the diaphragm is usually necessary to control the bleeding).
Postoperative management:
- Chest tubes may be removed if the lung is fully expanded and drainage volumes decrease below 20 to 50cc during a 24 hour period.
Prognosis:
- Good.
Recommend this site:


