
Pectus excavatum repair
General information:
- A funnel located mostly in the distal part of the sternum.
- Aetiology is still unclear. There is contiguity to a mechanical instability of the sternum and an overgrowth of the rib cartilages.
- 90% are noticeable within the first year of life.
- Occurs more frequently in boys (ratio: 3:1).
- In the asymmetrical funnel the depression is deeper on the right side and the sternum is twisted.
- In older patients (teenagers, adults) the posterior angulations of the most anterior portion of the osseous part of the ribs occur. That late stage should be avoided and the correction should be done earlier.
- Ages before 8 (growth of the lungs before 8) and around 14 (the implant stabilizes the thorax in the second period of increased growth) the are preferable.
- Mitral - valve prolapse is and slight valve insufficiencies are seen (compression and shifting of the heart to the left).
- 15 - 20% show additional musculoskeletal abnormalities like scoliosis.
- 37% have family histories.

Typical funnel chest
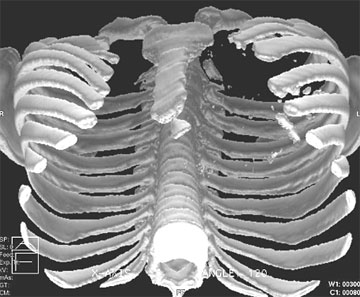
CT – 3D reconstruction
Symptoms:
- Pectus excavatum is well tolerated in infancy and childhood.
- Psychological stress.
- Palpitations.
- Arrhythmias and tachyarrhythmia’s.
- In cases of severe heart shift reduced stroke volume. Increased cardiac output is achieved primarily by increased heart rate because of the limited stroke volume.
- Pain in the area of the funnel.
- Exercise intolerance.
Preoperative workout; investigations:
- Thoracic X-ray, CT scan or MRI. Determination of a funnel chest index (Vertebral Index or Fronto - sagittal Index). The physiological rage of the vertebral index is between 15 and 25.
- Heart – Ultrasound to detect insufficiencies or mitral valve prolapse.
- ECG (duration of 24h and in different postures).
- Pulmonary function.
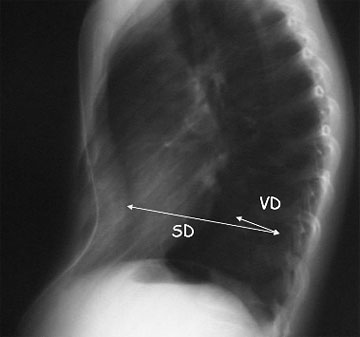
Vertebral Index: Vertebral Diameter (VD) x 100 / Sagittal Diameter (SD) + VD.
Indications for operation:
- Psychological stress.
- Arrhythmias, valve insufficiencies.
- Exercise impairment.
- Vertebral index above 26 or a Haller Index above 3.2.
Operation/Operation steps:
Possibilities of correction:
- The minimally invasive correction using an individually curved C–shaped steel bar with a single lateral stabilizer to elevate the sternum (Nuss-technique). The new generation implant is designed as one piece and stabilizer dislocation is not possible. Via two lateral incisions the bar is placed behind the sternum at the area of the deepest point of the funnel. In older patients two bars, "osteotomies" of calcified rib cartilage as well as a partial horizontal sternotomy at the upper median edge of the funnel may be necessary (exended modified procedure – Rokitansky).
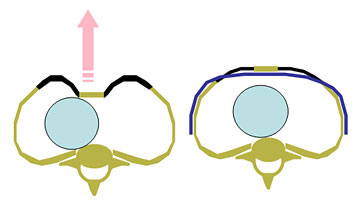
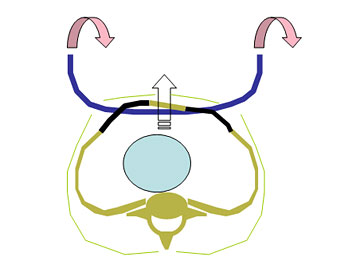
Principle of the minimally invasive pectus excavatum repair:
The new generation PS-Implant:

- If possible meet the requirements for single lung ventilation.
- Measurement from medioaxillary to medioaxillary line at the level of the deepest part of the funnel. Determination of the bar length (1 inch less of the measured distance).
- Two short (oblique) incisions in the medioaxillary line and subcutaneous mobilization in that area. For safety and technical reasons a third median incision below the processus xyphoideus that divides the linea alba is sometimes performed (Rokitansky). From that incision a retrosternal mobilization, long lasting intraoperative elevation of the sternum and thoracoscopy is performed. Thoracoscopy (e.g.: 5 mm port) is performed additionally from the right lateral incision.
Thoracoscopy:

- For optimal bar placement the intercostal space should be perforated within the edge of the funnel using a special “sword like” instrument. Caution: lesion of the arteria thoracica interna; lesion of the lungs or the pericardial sack or the heart. Visualization using the thoracoscopy is necessary. Visualization of the left intercostal perforation may be difficult because of the heart. Via the additional median subxiphoidal incison the tip of the preparation instrument may be guided additionally by the surgeons finger tip.
Way of preparation:

- A strong tape (e.g. 4mm Mersilene®) is fixed to the tip of the preparation instrument on one side and the end of the C – shaped bar on the other. The tape is covered by a silicone – tube to achieve atraumatic passage of the implant through the intercostal muscles.
End of the Bar covered by a silicone tube to guarantee atraumatic intercostal passage:

- The preparation instrument is pulled back and the bar is positioned behind the sternum with both ends looking to the front.

- Afterwards the bar is twisted (180°) using special instruments and fixed with sutures to the lateral thoracic muscles. The ends of the PS – Implant are positioned under the edge of the latissimus dorsi muscle. Using tow bars the upper one needs to be positioned under the pectoralis major muscle. Some surgeons prefer the fixation with sutures going around the rib.
- Chest tubes are used for drainage. If an additional median incision was performed, a single chest tube may be placed in the anterior mediastinum draining both opened pleural spaces.
- Analgetics are especially necessary in the first postoperative week (piritramid 0,1mg/kg BW/h or the pain-pump). The patient should start with breathing exercises as soon as possible.
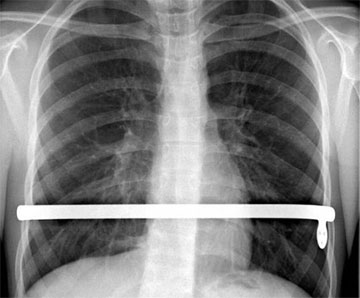
PS – Implant with the integrated stabilizer
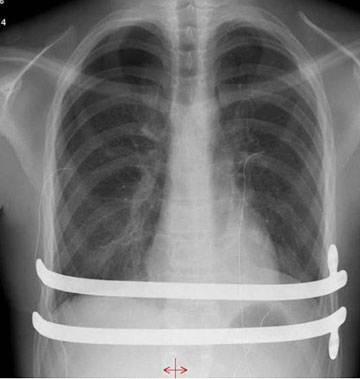
Two PS – Implants with integrated stabilizers (metal – metal touch, sometimes seen in the former generations is avoided – see below)
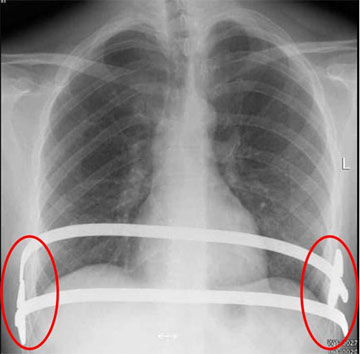
Possible “metal – metal touch” should be avoided
The bar should stay in place for at least two to three years. The advantage of this technique is the shorter duration of the operation. The hospitalization period and postoperative restriction on physical activity is shortened. Difficulties may occur if this technique is used on patients suffering from extremely asymmetric and narrow funnel (sometimes cosmetically poor result because of a protrusion on the parasternal area of the left thorax).
The “classic” technique (Ravitch – Welsh – Rehbein) elevating the sternum by partial bilateral resection of the elongated rib cartilages (mostly: rib 3. to rib 7.), sternotomy (wedge osteotomy) and stabilization using the Rehbein metal struts. The operation should not be performed below the age of 4 (possible impairment of the chest growing caused by a lesion of the costochondral junction).
- Horizontal or medio-sagittal incision in the central area of the funnel.
- Mobilization and elevation of the skin together with the major pectorlis muscles.
- Determination of the rib cartilages to be resected and incision of the perichondral tubes anteriorly by electocautery. Especially in young patients do not resect the complete cartilage. Because of growth the osteochondral junction should not be destroyed. Pleural lesions are most commonly performed on the 3rd or 4th right ribs. Caution must be paid to avoid a lesion of the internal mammaric vessels.
- Divide the xiphoid from the lower sternum.
- Perform a partial horizontal wedge osteotomy at the level above the last deformed cartilage. For blood hemostasis, fibrin - coated collagen patch may be used.
Wedge osteotomy

- Fixation of the osteotomy inducing the elevation of the sternum using wire sutures.
- Bilateral insertion of the Rehbein struts into the bone marrow of one or two pairs of ribs (e.g. 3rd or 4th ribs). The osteochondral junction of the rib should not be destroyed (growth impairment!). The Rehbein struts are medially joined to each other by wire and/or non - resorbable sutures creating a metal arch anterior to the sternum.
- The sternum is sewn to the artificial Rehbein – strut - arch to secure it in a forward position.
- The xiphoid is fixed again to the sternum and the pectorlis muscles are approximated and sewn in the middle above the elevated sternum. If tension prevents complete approximation, a patch (e.g. Gore soft tissue@) should be used.
- A submuscular and/or subcutaneous suction drain may be placed for two postoperative days.
- The Rehbein struts should stay in place for at least 6 months.
Correction using Rehbein struts

- The rib cartilage is remodelled after a period of about 2 months. Compared to the minimal invasive technique this is a more radical approach and its acceptance is limited. However there are still patients suffering a from highly asymmetrical and/or very stiff funnel chest (e.g. adult patients) who benfit more from the Ravitch – Welsh – Rehbein technique. Especially in mixed forms (pectus carinatum and excavatum) the techniques may be combined (resection of rib cartilage in the carinatum area and elevation using the retrosternal bar in the excavatum area).
- A plastic cushion may be implanted for cosmetic reasons, but due to the growth the results are uncertain. Due to the remaining mediastinal shift this technique can not be recommended.
Postoperative management:
- Remove pleural drainage in the first postoperative week (quantity of drained fluid less than 100cc) and the suction drainage around the second postoperative day.
- Intravenous analgetics (e.g. Dipidolor@ - piritramid 0,1mg/kg BW/h) and antibiotics.
- Start respiratory exercises as early as possible.
- Full muscular training after complete healing once a mechanically resistant scar has developed (especially thoracic and abdominal muscles; swimming is recommended) starting in the second postoperative month.
Prognosis:
- Recurrence rate up to 5 to 10 % (higher in patients with Marfan syndrome).
- Delaying the surgery until the children have begun the pubertal growth spurt is beneficial.
 Pediatric Surgery Digest
Pediatric Surgery Digest
Currently, the international textbook "Pediatric Surgery Digest" (ISBN 978-3-030-80410-7; ISBN 978-3-030-80411-4 (eBook) https://doi.org/10.1007/978-3-030-80411-4) has been published in its 2nd edition by Springer-Verlag. The editor is Zarachias Zachariou. The work covers the entire field of pediatric and adolescent surgery in a streamlined manner, so that one can quickly orientate oneself in the clinical routine and get an overview. Alexander Rokitansky has written the chapter (16 / page 187-234) of the entire thoracic surgery.


